
National
Federal virus money slow to trickle to local public health
As the novel coronavirus began to spread through Minneapolis this spring, Health Commissioner Gretchen Musicant tore up her budget to find funds to combat the crisis. Money for test kits. Money to administer tests. Money to hire contact tracers. And yet even more money for a service that helps tracers communicate with residents in dozens of languages.
While Musicant diverted workers from violence prevention and other core programs to the COVID-19 response, state officials debated how to distribute $1.87 billion Minnesota received in federal aid.
As she waited, the Minnesota Zoo got $6 million in federal money to continue operations, and a debt collection company outside Minneapolis received at least $5 million from the federal Paycheck Protection Program, according to federal data.
It was not until Aug. 5 — months after Congress approved aid for the pandemic — that Musicant’s department finally received $1.7 million, the equivalent of $4 per Minneapolis resident.
“It’s more a hope and a prayer that we’ll have enough money,” Musicant said.
Since the pandemic began, Congress has set aside trillions of dollars to ease the crisis. A joint Kaiser Health News and Associated Press investigation finds that many communities with big outbreaks have spent little of that federal money on local public health departments for work such as testing and contact tracing. Others, like in Minnesota, were slow to do so.
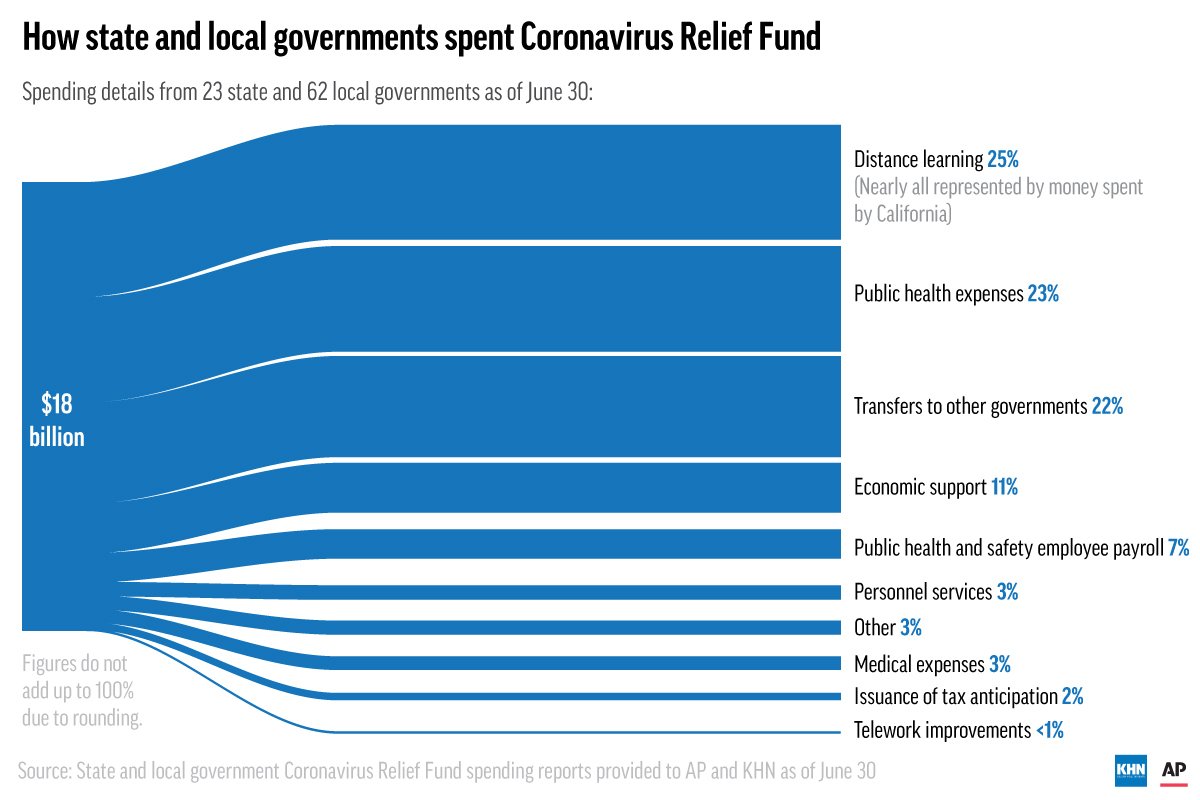
For example, the states, territories and 154 large cities and counties that received allotments from the $150 billion Coronavirus Relief Fund reported spending only 25% of it through June 30, according to reports that recipients submitted to the U.S. Treasury Department.
Many localities have deployed more money since that June 30 reporting deadline, and both Republican and Democratic governors say they need more to avoid layoffs and cuts to vital state services. Still, as cases in the U.S. top 5 million and deaths soar past 165,000, Republicans in Congress are pointing to the slow spending to argue against sending more money to state and local governments to help with their pandemic response.
“States and localities have only spent about a fourth of the money we already sent them in the springtime,” Senate Majority Leader Mitch McConnell said Tuesday. Congressional Democrats’ efforts to get more money for states, he said, “aren’t based on math. They aren’t based on the pandemic.”
Negotiations over a new pandemic relief bill broke down last week, in part because Democrats and Republicans could not agree on funding for state and local governments.
KHN and the AP requested detailed spending breakdowns from recipients of money from the Coronavirus Relief Fund — created in March as part of the $1.9 trillion CARES Act — and received responses from 23 states and 62 cities and counties. Those entities dedicated 23% of their spending from the fund through June to public health and 7% to public health and safety payroll.
An additional 22% was transferred to local governments, some of which will eventually pass it down to health departments. The rest went to other priorities, such as distance learning.
So little money has flowed to some local health departments for many reasons: Bureaucracy has bogged things down, politics have crept into the process, and understaffed departments have struggled to take time away from critical needs to navigate the red tape required to justify asking for extra dollars.
“It does not make sense to me how anyone thinks this is a way to do business,” said E. Oscar Alleyne, chief of programs and services at the National Association of County and City Health Officials. “We are never going to get ahead of the pandemic response if we are still handicapped.”
Last month, KHN and the AP detailed how state and local public health departments across the U.S. have been starved for decades. Over 38,000 public health worker jobs have been lost since 2008, and per capita spending on local health departments has been cut by 18% since 2010. That’s left them underfunded and without adequate resources to confront the coronavirus pandemic.
“Public health has been cut and cut and cut over the years, but we’re so valuable every time you turn on the television,” said Jan Morrow, the director and 41-year veteran of Ripley County health department in rural Missouri. “We are picking up all the pieces, but the money is not there. They’ve cut our budget until there’s nothing left.”
POLITICS AND RED TAPE
Why did the Minneapolis health department have to wait so long for CARES Act money?
Congress mandated that the Coronavirus Relief Fund be distributed to states and local governments based on population. Minneapolis, with 430,000 residents, missed the threshold of 500,000 people that would have allowed it to receive money directly.
The state of Minnesota, however, received $1.87 billion, a portion of which was meant to be sent to local communities. Lawmakers initially sent some state money to tide communities over until the federal money came through — the Minneapolis health department got about $430,000 in state money to help pay for things like testing.
But when it came time to decide how to use the CARES Act money, lawmakers in Minnesota’s Republican-controlled Senate and Democratic-controlled House were at loggerheads.
Myron Frans, commissioner of Minnesota Management and Budget, said that disagreement, on top of the economic crisis and pandemic, left the legislature in turmoil.
Then following the police killing of George Floyd, the city erupted in protests over racial injustice, making a difficult situation even more challenging.
Democratic Gov. Tim Walz favored targeting some of the money to harder-hit communities, a move that might have helped Minneapolis, where cases have surged since mid-July. But lawmakers couldn’t agree. Negotiations dragged on, and a special session merely prolonged the standoff.
Finally, the governor divvied up the money using a population-based formula developed earlier by Republican and Democratic legislative leaders that did not take into account COVID-19 caseloads or racial disparities.
“We knew we needed to get it out the door,” Frans said.
The state then sent hundreds of millions of dollars to local communities. Still, even after the money got to Minneapolis a month ago, Musicant had to wait as city leaders made difficult choices about how to spend the money as the economy cratered and the list of needs grew.
“Even when it gets to the local government, you still have to figure out how to get it to local public health,” Musicant said.
Meanwhile, some in Minneapolis have noticed a lack of services. Dr. Jackie Kawiecki has been providing help to people at a volunteer medical station near the place where Floyd was killed — an area that at times has drawn hundreds or thousands of people per day. She said the city did not do enough free, easy-to-access testing in its neighborhoods this summer.
“I still don’t think that the amount of testing offered is adequate, from a public health standpoint,” Kawiecki said.
A coalition of groups that includes the National Governors Association has blamed the spending delays on the federal government, saying the final guidance on how states could spend the money came late in June, shortly before the reporting period ended. The coalition said state and local governments had moved “expeditiously and responsibly” to use the money as they deal with skyrocketing costs for health care, emergency response and other vital programs.
New York’s Nassau County was among six counties, cities and states that had spent at least 75% of its funds by June 30.
While most of the money was not spent before then, the National Association of State Budget Officers says a July 23 survey of 45 states and territories found they had allocated, or set aside, an average of 74% of the money.
But if they have, that money has been slow to make it to many local health departments.
As of mid-July in Missouri, at least 50 local health departments had yet to receive any of the federal money they requested, according to a state survey. The money must first flow through local county commissioners, some of whom aren’t keen on sending money to public health agencies.
“You closed their businesses down in order to save their people’s lives and so that hurt the economy,” said Larry Jones, executive director for the Missouri Center for Public Health Excellence, an organization of public health leaders. “So they’re mad at you and don’t want to give you money.”
The winding path federal money takes as it makes its way to states and cities also could exacerbate the stark economic and health inequalities in the U.S. if equity isn’t considered in decision-making, said Wizdom Powell, director of the University of Connecticut Health Disparities Institute.
“Problems are so vast you could unintentionally further entrench inequities just by how you distribute funds,” Powell said.
‘EVERYTHING FELL BEHIND’
The amounts eventually distributed can induce head-scratching.
Some cities received large federal grants, including Louisville, Kentucky, whose health department was given $42 million by April, more than doubling its annual budget. Because of the way the money was distributed, Louisville’s health department alone received more money from the CARES Act than the entire government of the city of Minneapolis.
Philadelphia’s health department was awarded $100 million from a separate fund from the Centers for Disease Control and Prevention.
Honolulu County, where cases have remained relatively low, received $124,454 for every positive COVID-19 case it had reported as of Aug. 9, while El Paso County in Texas got just $1,685 per case. Multnomah County, Oregon — with nearly a quarter of its state’s COVID-19 cases — landed only 2%, or $28 million, of the state’s $1.6 billion allotment.
Rural Saline County in Missouri received the same funding as counties of similar size, even though the virus hit the area particularly hard. In April, outbreaks began tearing through a Cargill meatpacking plant and a local factory. By late May, the health department confirmed 12 positive cases at the local jail.
Tara Brewer, Saline’s health department administrator, said phone lines were ringing off the hook, jamming the system. Eventually, several department employees handed out their personal cell phone numbers to take calls from residents looking to be tested or seeking care for coronavirus symptoms.
“Everything fell behind,” Brewer said.
The school vaccination clinic in April was canceled, and a staffer who works as a Spanish translator for the Women, Infants and Children nutritional program was enlisted to contact trace for additional coronavirus exposures. All food inspections stopped.
It was late July when $250,000 in federal CARES Act money finally reached the 11-person health department, Brewer said — four months after Congress approved the spending and three months after the county’s first outbreak.
That was far too late for Brewer to hire the army of contact tracers that might have helped slow the spread of the virus back in April. She said the money already has been spent on antibody testing and reimbursements for groceries and medical equipment the department had bought for quarantined residents.
Another problem: Some local health officials say that the laborious process required to qualify for some of the federal aid discourages overworked public health officials from even trying to secure more money and that funds can be uneven in arriving.
Lisa Macon Harrison, public health director for Granville Vance Public Health in rural Oxford, North Carolina, said it’s tough to watch major hospital systems — some of which are sitting on billions in reserves — receive direct deposits, while her department received only about $122,000 through three grants by the end of July. Her team filled out a 25-page application just to get one of them.
She is now waiting to receive an estimated $400,000 more. By contrast, the Duke University Hospital System, which includes a facility that serves Granville, already has received over $67.3 million from the federal Provider Relief Fund.
“I just don’t understand the extra layers of onus for the bureaucracy, especially if hundreds of millions of dollars are going to the hospitals and we have to be responsible to apply for 50 grants,” she said.
The money comes from dozens of funds, including several programs within the CARES Act. Nebraska alone received money from 76 federal COVID relief funding sources.
Robert Miller, director of health for the Eastern Highlands Health District in Connecticut, which covers 10 towns, received $29,596 of the $2.5 million the state distributed to local departments from the CDC fund and nothing from CARES. It was only enough to pay for some contact tracing and employee mileage.
Miller said that he could theoretically apply for a little more from the Federal Emergency Management Agency, but that the reporting requirements — which include collecting every receipt — are extremely cumbersome for an already overburdened department.
So he wonders: “Is the squeeze worth the juice?”
Back in Minneapolis, Musicant said the new money from CARES allowed the department to run a free COVID-19 testing site Saturday, at a church that serves the Hispanic community about a mile from the site of Floyd’s killing.
It will take more money to do everything the community needs, she says, but with Congress deadlocked, she’s not sure they’ll get it anytime soon.
Smith is a writer for The Associated Press, and Weber, Recht and Ungar are writers for KHN. AP writers Camille Fassett and Steve Karnowski contributed to this report.
This story is a collaboration between The Associated Press and KHN, which is a nonprofit news service covering health issues. It is an editorially independent program of the Kaiser Family Foundation. KHN is not affiliated with Kaiser Permanente.
